


🤯 Burning Hours After Contact? Dermatitis vs. Nerve Pain (Vulvodynia) | Dr. Farzana Khan
🤯 Burning Hours After Contact? Dermatitis vs. Nerve Pain (Vulvodynia) | Dr. Farzana Khan

Can the O-Shot help with burning or irritation? | WHC Clinical FAQ
Tacrolimus
Tolerability
Specialist adjunct
Women’s Health Clinic FAQ
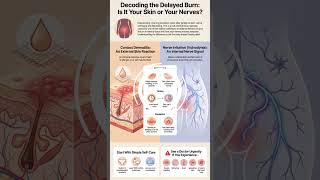
Why does tacrolimus ointment often cause an intense burning sensation during initial applications, and how is this managed?
Tacrolimus burning can be frightening, especially on fragile vulval skin, but it needs to be interpreted in the context of indication, inflammation and severity.
Direct answer
Tacrolimus can burn on inflamed or fragile vulval skin during early use; clinicians manage this by confirming indication, reducing irritation, adjusting use and stopping or reviewing if symptoms are severe.
The safest answer explains why burning may happen, how clinicians adjust treatment and when symptoms mean the plan should be reviewed.
Educational only. Suitability and next steps should be confirmed after consultation. Results vary. Not a cure.

Tacrolimus tolerance
At a glance
These are the main points to understand before deciding whether symptoms need self-care, prescribed treatment, specialist review or urgent advice.
At a glance
Clinical summary
Main area
Treatment tolerance
Care pattern
Review-led
Watch for
Severe burning
Next step
Medication review
Important safety note
New, changing or painful skin symptoms should be assessed rather than repeatedly self-treated, especially if there is bleeding, ulceration, urinary change or rapid scarring.
Symptoms
Treatment
Review
Safety
Detailed answer
The clinical answer
The useful answer starts by separating active inflammation, established scarring, irritant symptoms, infection, GSM overlap, urinary involvement and non-standard treatment claims.
Direct answer
The reader wants to understand tacrolimus burning, whether it is expected, and when the treatment needs modification or review.
Scarring
Treatment
Follow-up
Direct answer
Start with the exact concern and the anatomy involved, because vulval skin, vaginal tissue, the introitus, foreskin, meatus and urethra need different thinking.
Why burning happens
Symptoms should be interpreted alongside appearance, fissures, pain, urinary features, treatment history and whether the problem is new or changing.
When tacrolimus is considered
Treatment choices should keep prescribed anti-inflammatory care central and frame adjunctive or supportive options realistically.
Practical tolerance steps
Follow-up matters when symptoms persist, recur, affect sex or urination, or change vulval or penile architecture.
How the research shapes the answer
Evidence-Based Efficacy: Tacrolimus is robustly used as a second-line or steroid-sparing treatment for chronic inflammatory dermatoses, including atopic dermatitis and refractory vulval lichen sclerosus. Lichen Sclerosus Outcomes: Clinical trials comparing topical tacrolimus to ultrapotent.
The research synthesis shaped the structure, while final wording avoids complete treatment framing, sexual-wellness marketing, treatment ranking, device hype and promises of tissue reversal.
Patient safety
Why this distinction matters
This distinction matters because lichen sclerosus can be missed, over-simplified or overtreated when symptoms are reduced to itching, dryness, cosmetic concern or sexual discomfort alone.
It normalises context
Some burning can occur early, especially on inflamed skin.
It protects patients
Severe, worsening or intolerable burning should not be endured.
It keeps treatment hierarchy clear
Tacrolimus is usually a specialist adjunct or alternative.
It reduces confusion
Burning does not automatically prove allergy or treatment failure.
Calm, precise care
Good lichen sclerosus information should reduce shame and confusion while making review thresholds clearer.
The right next step may be reassurance, swabs, biopsy, steroid review, GSM care, urology, paediatric review, specialist vulval care or urgent advice.
Considerations
What to consider
A consultation should clarify diagnosis, current treatment, symptom control, self-care, escalation signs and whether specialist review is needed.
Consultation priorities
Track symptoms, visible change, fissures, pain, urine stinging, urinary stream, treatment use, irritants, sexual discomfort, scarring and whether symptoms are improving.
Examination
Treatment
Follow-up
Confirm indication
The reason for tacrolimus should be clear.
Reduce irritants
Washes, friction and active inflammation can worsen stinging.
Review application
Amount, frequency and timing may need adjustment.
Escalate severe symptoms
Marked pain, swelling, ulceration or worsening needs review.
What not to assume
Do not assume every flare is thrush, every white patch is lichen sclerosus, or every symptom can be solved with a procedure.
Initial Application (Days 1-7): Patients should expect a pronounced burning or stinging sensation immediately following the application of the ointment. Adaptation Phase (Weeks 1-3): As the skin barrier begins to heal and local mast.
Common concerns and myths
Common misconceptions
These corrections keep the page practical, cautious and less vulnerable to online overclaims.
Myth: Tacrolimus burning always means allergy
Reality: symptoms, examination and treatment response matter more than assumptions.
Myth: Calcineurin inhibitors replace standard LS treatment
Reality: symptoms, examination and treatment response matter more than assumptions.
Myth: Severe burning should simply be endured
Reality: symptoms, examination and treatment response matter more than assumptions.
Diagnosis comes first
Similar symptoms can come from lichen sclerosus, thrush, GSM, vitiligo, lichen planus, irritant dermatitis, urinary infection or pelvic-floor guarding.
Treatment should stay proportionate
Supportive care, prescribed treatment, hormones, surgery, dilators and adjunctive options have different roles and should not be blurred together.
Safety checklist
Safety checklist
Use these checks to decide whether symptoms are more suitable for routine review, specialist review or urgent advice.
Is the diagnosis clear?
Persistent or recurrent symptoms should not be repeatedly treated without examination.
Is disease active?
Itch, fissures, soreness, texture change or new whitening may suggest active inflammation.
Is function affected?
Pain with sex, urine stinging, narrowing, stream change or daily discomfort should be discussed.
Are red flags present?
Bleeding, non-healing ulcers, new lumps, rapid change or urinary retention need prompt advice.
More reassuring signs
The situation is more reassuring when symptoms are improving, diagnosis is clear, treatment technique is understood and follow-up is planned.
Known plan
Review booked
Reasons to seek advice
Seek advice for severe pain, unexplained bleeding, non-healing ulcers, new lumps, urinary stream change, retention, fever, spreading redness or safeguarding concerns.
Ulcer
Urinary change
When to escalate
When to seek medical help
Some symptoms should not be managed with self-care, online advice or repeat treatment alone.
Use NHS 111 online
Changing skin
A new lump, non-healing ulcer, bleeding, rapid scarring or marked colour or texture change should be assessed.
Pain or urinary change
Severe pain, urine retention, stream change, spraying or persistent urine stinging should be reviewed.
Infection or safeguarding concerns
Fever, spreading redness, discharge, child safeguarding concerns or unexplained injury patterns need appropriate advice.
Emergency symptoms
Call 999 for life-threatening symptoms such as collapse, chest pain, breathing difficulty or severe allergic reaction.
Use NHS 111 for urgent advice or call 999 in a life-threatening emergency. This page is educational and does not replace individual medical assessment.
Additional clinical context
How to use this answer
Use this page to separate active lichen sclerosus, established scarring, irritant symptoms, urinary involvement, GSM overlap and treatment marketing. The safest next step depends on symptoms, examination and whether the concern is changing.What to bring to review
Helpful details include symptom timing, itch, soreness, fissures, urine stinging, urinary stream, visible change, sexual discomfort, treatment use, irritants, previous swabs or biopsy, and whether symptoms are improving or worsening.Regulatory resources
Authoritative resources
These resources support cautious advice on tacrolimus, calcineurin inhibitors, vulval burning and specialist lichen sclerosus treatment choices.
Next step
Book a confidential consultation
A consultation can review whether tacrolimus is appropriate, whether burning is expected, and whether treatment should be adjusted or stopped.
▶ View Research Sources (12 Sources)
These 12 source names are selected from 12 display-ready sources, with a raw audit trail of 46 imported records. Additional reviewed material included UK clinical guidance, peer-reviewed clinical papers, evidence reviews; duplicate, low-relevance and non-clinical records were removed before display.
Educational only. This information is for education only and is not a substitute for professional medical advice, diagnosis or treatment. Results vary. Not a cure.