Content approved by: Dr Farzana Khan, MD, MRCGP, DFFP — Specialist in vaginal health with 20+ years’ medical experience across dermatology and gynaecology. Care is balanced, evidence-aware, and patient-centred.
Dr Farzana Khan qualified as an MD from the University of Copenhagen in 2003. She has worked in dermatology and obstetrics & gynaecology across the North of England and completed her MRCGP (CCT, 2013) and the Diploma of the Faculty of Sexual & Reproductive Health (2013).
Her clinical focus is vaginal health—including dryness/GSM, sexual function concerns, lichen sclerosus, and comfort or volume changes. She explains conservative and medical options first, then discusses regenerative or aesthetic procedures where appropriate.
Dr Farzana is a key opinion leader on women’s intimate health and been featured in the press including the daily mail and on BBC radio. Dr Farzana also trains clinicians as a Trainer with Neauvia, NuV Laser, Asclepion Juliet Laser, and RegenLab. Ongoing CPD includes IMCAS, CCR, ACE and expert training in intimate fillers, PRP and polynucleotides.
Authored and medically reviewed by Dr Farzana Khan. Last updated: 1 November 2025.
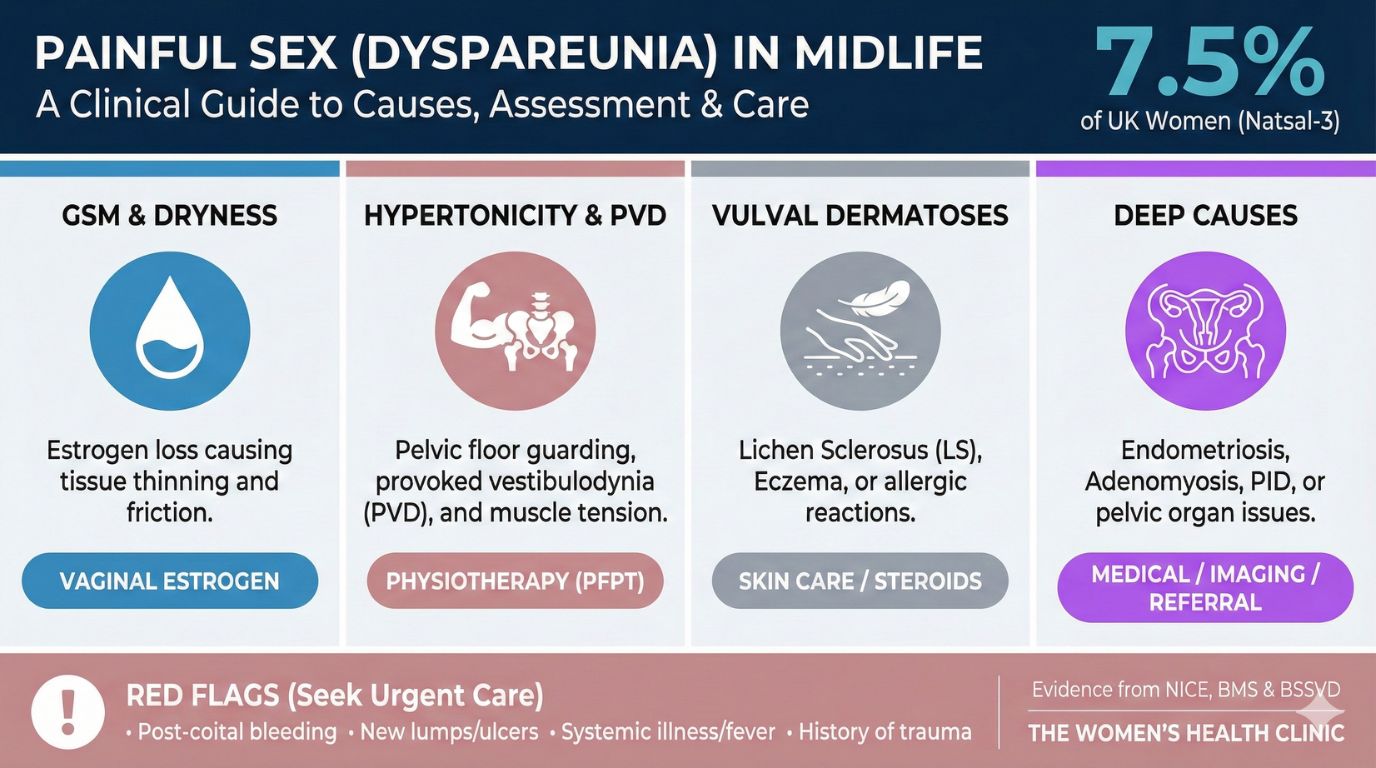
Understanding Painful Sex: A Gentle Guide to Causes and Solutions
If you are experiencing pain during sex, the first and most important thing to know is that you are not alone, and it is not your fault. Painful sex, known clinically as dyspareunia, is a common medical issue that affects countless women—research shows approximately 1 in 10 women in Britain report experiencing it.
It is a genuine physical condition, not a personal failing. Clinicians now recognise this interconnected experience under the term Genito-pelvic pain/penetration disorder (GPPPD), validating that your physical and emotional responses are linked. This guide is designed to demystify the topic and help you find the path to comfortable intimacy.
Key Takeaways
- You Are Not Alone: Dyspareunia affects 1 in 10 women and is a valid medical condition.
- Location Matters: Distinguishing between "entrance pain" and "deep pain" is the first step to accurate diagnosis.
- Multimodal Treatment: The best results often come from combining medical, physical, and psychological therapies.
- Safety First: Be cautious with "rejuvenation" procedures; prioritize evidence-based care.
Table of Contents
1.0 The First Step: Identifying Your Pain
The first step in finding a solution is accurately describing your pain. Is it at the entrance (superficial) or deeper inside? This distinction provides crucial clues.
Pain at the Entrance
Feels like: Sharp, stinging, "paper cut," or "sandpaper" rawness.
When: On initial touch, tampon insertion, or smear tests.
Deep Pelvic Pain
Feels like: Deep ache, cramping, "bruised" feeling, or "collision" pain.
When: During deep thrusting, certain positions, or aching after sex.
 Book Appointment
Book Appointment 2.0 Common Causes of Pain at the Vaginal Entrance
Pain at the introitus often relates to the health of the skin, muscles, and nerves. Here are the most common drivers:
Hormonal Changes (GSM)
Low oestrogen (menopause, breastfeeding, pill) causes thinning and dryness. The combined pill can also increase SHBG, lowering testosterone and causing tissue fragility.
Nerve Hypersensitivity (PVD)
Nerves at the vestibule misinterpret light touch as burning pain. The skin often looks normal. Diagnosed via the "Q-Tip test" (pain at 5 & 7 o'clock).
Vaginismus
A protective, involuntary guarding reflex where muscles spasm, creating a "wall." It is not something you can consciously control.
Skin Conditions & Scars
Lichen Sclerosus (white patches), Dermatitis (irritants), or rigid scar tissue from childbirth tears/episiotomy.
3.0 Understanding Aches and Pains Deeper Inside
Deep pain during thrusting is often related to pelvic organs or deep muscle layers.
[Image of endometriosis vs adenomyosis uterus comparison]- Endometriosis & Adenomyosis: Tissue growing outside the uterus (Endo) or within the muscle wall (Adeno) causes "collision dyspareunia." Dyschezia (painful bowel movements) during periods is a key sign.
- Deep Pelvic Floor Tension: Trigger points in deep muscles (like the Obturator Internus) cause referred pain to the hip/buttock and a lingering "bruised" sensation.
- Organ Issues: Ovarian cysts or fibroids can cause sharp/aching pain when compressed during intercourse.
Need help identifying the cause?
Get Support4.0 Your Path to Comfortable Intimacy
The best results come from a multimodal approach combining home strategies, medical care, and psychological support.
A. Foundational Steps (Home Care)
- Smart Lubrication: Use high-quality lube to reduce friction.
- Positions: Try "Woman-on-top" or "Spooning" to control depth.
- Traffic Light System: Green (Go), Amber (Slow), Red (Stop) to build trust.
- Avoid Irritants: Use plain water or emollients; avoid fabric softeners.
B. Medical & Physical Therapies
[Image of pelvic floor muscles and obturator internus]- Topical Hormones: Vaginal Oestrogen or DHEA (dual action) to restore tissue thickness and elasticity.
- Pelvic Health Physio: Focuses on "Down-Training" (relaxing) muscles using Biofeedback.
- Vaginal Dilators: Tools for neuromuscular desensitization. The "Clock Face" massage releases knots. Vibrating dilators use the "Gate Control Theory" to block pain signals.
C. Psychological Support
The brain can learn a "Fear-Pain Cycle." Mindfulness and Graded Exposure (Visual -> Touch -> Passive -> Active) help retrain the nervous system.
D. Caution: Advanced Procedures
Procedures like Laser/RF and PRP are sometimes used when first-line treatments fail. However, proceed with caution:
- FDA Warning: Warns against energy-based devices for "rejuvenation" due to burn risks.
- NICE Guidance: States evidence for long-term safety is "inadequate" for routine use.
Reclaim Your Confidence
Painful sex is a treatable medical condition. Taking the first step towards help is courageous.
5.0 Taking the Next Step: Seeking a Diagnosis
A normal scan or swab does not mean the pain is "in your head." Your experience is valid. Here is what to expect at a specialist consultation:
- Pain Map: A compassionate conversation to map where and when it hurts.
- Q-Tip Test: A gentle external check for nerve sensitivity.
- Single Digit Exam: Internal exams are often done with one finger to check muscles, avoiding the speculum initially.
Disclaimer: This content is for informational purposes only and does not constitute medical advice. Consult a healthcare professional for diagnosis and treatment.