Content approved by: Dr Farzana Khan, MD, MRCGP, DFFP — Specialist in vaginal health with 20+ years’ medical experience across dermatology and gynaecology. Care is balanced, evidence-aware, and patient-centred.
Dr Farzana Khan qualified as an MD from the University of Copenhagen in 2003. She has worked in dermatology and obstetrics & gynaecology across the North of England and completed her MRCGP (CCT, 2013) and the Diploma of the Faculty of Sexual & Reproductive Health (2013).
Her clinical focus is vaginal health—including dryness/GSM, sexual function concerns, lichen sclerosus, and comfort or volume changes. She explains conservative and medical options first, then discusses regenerative or aesthetic procedures where appropriate.
Dr Farzana is a key opinion leader on women’s intimate health and been featured in the press including the daily mail and on BBC radio. Dr Farzana also trains clinicians as a Trainer with Neauvia, NuV Laser, Asclepion Juliet Laser, and RegenLab. Ongoing CPD includes IMCAS, CCR, ACE and expert training in intimate fillers, PRP and polynucleotides.
Authored and medically reviewed by Dr Farzana Khan. Last updated: 1 November 2025.
Understanding Painful Sex (Dyspareunia) in Midlife
Painful sex (dyspareunia) is common and can have many overlapping causes, especially around perimenopause and menopause. [1]
It is real, legitimate pain—not "in your head"—and you deserve thorough, compassionate assessment. [2–4]
This guide explains how clinicians think about painful sex, common causes, red flags, what happens in an assessment, and the kinds of management options UK guidelines support. It is based on current evidence from NICE, the British Menopause Society (BMS), BSSVD, ISSVD/ISSWSH and related bodies. [1,3,4,6,8–11,15]
Key Takeaways
- Painful sex is common in UK women and strongly linked with lower sexual, emotional and relationship wellbeing. [2]
- Clinicians separate entry (at or near the opening) and deep pain to guide possible causes and tests. [3,5,10]
- Common causes include menopause-related changes, pelvic-floor tension, vulval skin conditions, infections and endometriosis. [1,3,4,6,8,10,11,15]
- First-line care typically combines pelvic-health physiotherapy, vaginal oestrogen, skin care and psychosexual support, tailored to the cause(s). [1,4–6,8–10,15]
- Some procedures (for example, vaginal "rejuvenation" lasers) lack strong evidence and carry known risks, so are not recommended as routine treatment. [7,8,14]
Table of Contents
- What is painful sex (dyspareunia)?
- How common is painful sex and why does it matter?
- Common causes of painful sex around midlife
- When is painful sex a red flag?
- What happens at a painful sex assessment?
- Treatment options based on the cause
- Adjuncts, procedures and what to be cautious about
- Getting the right support and specialist care
- Living with painful sex
- Questions you might ask your clinician
- Key research gaps
- Key statistics at a glance
- About this guide and the evidence
- References
- FAQs
1. What is Painful Sex (Dyspareunia)?
Painful sex (dyspareunia) means genital pain that happens in connection with sexual activity—before, during or after penetration. [3] Clinicians usually separate entry (introital) pain, felt at or near the vaginal opening, from deep pain felt higher up in the pelvis. This distinction matters because the likely causes and investigations differ. [3,5,10]
Common Terminology
- Vulvodynia: Longer-term vulval pain without a clearly identifiable cause.
- Vestibulodynia: Pain triggered by touch at the vestibule—the ring of tissue just inside the vaginal opening. [3]
- GPPPD: Genito-pelvic pain/penetration disorder (DSM-5 diagnosis) used when difficulties with penetration, pain, and pelvic-floor tightening come together. [3]
In midlife, painful sex often reflects more than one factor at once. For example, menopausal changes (genitourinary syndrome of menopause, GSM), pelvic-floor muscle tension, and past infections or childbirth-related scarring may all play a role. [1,3–5,8,10,15]
If you're unsure which type of pain you have, that's completely okay. Part of your clinician's role is to help you describe where it hurts and what it feels like, using accessible language. [3,8,9]
2. How Common is Painful Sex and Why Does it Matter?
Painful sex is common, particularly among women and people with a vagina in midlife, and it affects much more than the bedroom. [2] Understanding how widespread it is can help challenge feelings of isolation or shame. [2]
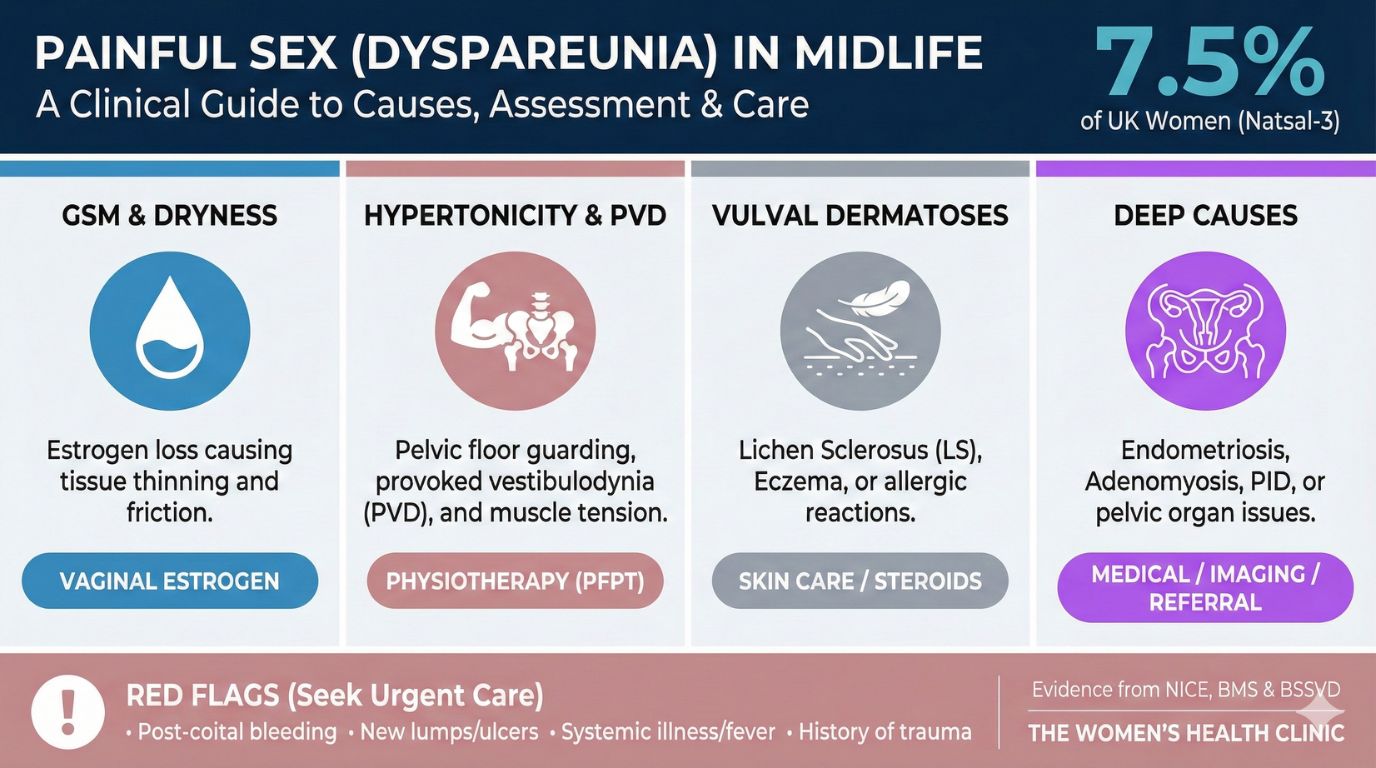
A large UK survey (Natsal-3) found that around 7.5% of sexually active women reported painful sex in the previous year. [2] Those who experienced pain were more likely to report lower sexual satisfaction, reduced desire, difficulties with arousal and orgasm, and worse mental and relationship wellbeing than women without pain. [2]
These findings highlight why guidelines emphasise proactive, empathetic enquiry rather than waiting for women to bring it up themselves, especially in menopause and sexual-health consultations. [1,4,6,8,10] Painful sex may be linked with conditions such as endometriosis, vulval dermatoses, infections, bladder pain syndrome, or pelvic-floor tension. But it can also create understandable fear, avoidance of intimacy, and knock-on strain within relationships. [3–6,8,10,11]
At The Women's Health Clinic you can also explore our information on menopause, vaginal dryness and sexual wellbeing to put these figures into context and prepare for conversations in clinic.
3. Common Causes of Painful Sex Around Midlife
Painful sex rarely has a single simple cause, particularly around perimenopause and menopause. [1,3–5,8,10,15] Clinicians use a "phenotype" approach: first asking whether pain is mainly at the entrance or deeper inside, then considering overlapping drivers. [3,5,8,10]
Menopause-Related Changes (GSM)
GSM refers to oestrogen-related changes that can affect the vulva, vagina and lower urinary tract. [1,4,13,15] Typical features include dryness, burning or itching, less natural lubrication and superficial pain with touch or penetration. Symptoms can appear after menopause, during perimenopause, in premature ovarian insufficiency, while breastfeeding, or with anti-oestrogen medications. [1,4,13,15] On examination, tissues may look pale, thin and more fragile, with loss of the normal folds (rugae) and sometimes small fissures or bleeding. [1,4,13,15]
Moisturisers and lubricants can be very helpful for comfort, but current evidence does not support saying they are "equivalent" to vaginal oestrogen for pain relief in GSM. [1,4,13,15]
PVD & Pelvic-Floor Tension
If your main pain is a sharp, burning, cutting or raw sensation exactly at the entrance—especially with first attempts at penetration, tampon use, or smear tests—clinicians think about provoked vestibulodynia (PVD) and related pelvic-floor tension. [3,5,9]
On gentle testing with a cotton swab, people with PVD often have focal tenderness at the lower part of the vestibule (often around 5–7 o'clock), even when the tissue looks normal. [3,5,9] Pelvic-floor muscles are frequently tight and tender at the same time, which can create a "guarding" response and make penetration feel impossible or very painful. [3,5,9]
Evidence and consensus recommend multimodal pelvic-floor physical therapy (PFPT)—including down-training, manual therapy, myofascial release, biofeedback, dilator work and education—as a first-line component of care. [5,8,9] A randomised trial found that PFPT led to greater improvements in pain and sexual function than topical lidocaine alone in people with PVD. [5] Night-time 5% lidocaine can still be helpful as part of combined care. [3,5,8,9]
Infections
Recurrent or persistent genital infections can cause burning pain with sex as well as discharge, odour or itching. [10] Common examples include thrush (candidiasis), bacterial vaginosis and sexually transmitted infections like chlamydia or gonorrhoea. [10]
Clinicians may examine the vulva and vagina, check vaginal pH or microscopy where available, and take swabs according to local sexual-health pathways. [10] Treatment follows antimicrobial guidelines. If pain remains after repeated infections have been treated, they will look for other contributors such as PVD or GSM. [1,4,5,8,10]
Vulval Dermatoses
Skin conditions affecting the vulva are a key, often under-recognised cause of soreness and painful sex. [8,10] These include:
- Lichen sclerosus (LS)—typically ivory-white plaques and fragile skin
- Lichen planus (LP)—glazed red areas or erosions
- Eczema/contact dermatitis/psoriasis—patterned or scaly plaques, often itchy [8,10]
Women may describe intense itching, soreness, fissures, or a feeling that the vulval shape is changing (for example, labial resorption or clitoral hood tightening), all of which can make touch and penetration painful. [8,10]
Guidelines recommend ultra-potent topical steroids as mainstay treatment for LS, with tailored regimens for LP, eczema and psoriasis. [8,10] Biopsy is advised for atypical or non-responding lesions, and patch testing may be offered if allergic contact dermatitis is suspected. Suspicious or non-healing areas should be urgently assessed via specialist vulval services because a small minority may represent pre-cancerous or cancerous change. [8,10]
Postpartum Trauma & Scars
After childbirth, especially if you had an episiotomy or tear, scar tissue at the entrance can remain tight or tender and cause pain exactly at the scar line with penetration. [8] This may combine with pelvic-floor tension and, during breastfeeding, GSM-like dryness due to low oestrogen. [1,4,8,15]
Approaches include scar desensitisation and massage, graded vaginal dilators, PFPT to address muscle tension, and topical oestrogen where appropriate in the context of lactation. [1,4,8,15] These are usually offered alongside gentle, trauma-informed conversations about fear of re-injury and rebuilding confidence after birth. [3,8]
Pelvic-Floor Hypertonicity
Pelvic-floor muscles can become over-recruited and tight in response to pain, stress, trauma, constipation, heavy exercise, or simply habit. [3,5,8,9] This can show up as difficulty tolerating penetration or even a speculum, burning or tightness at the entrance, or deep aching with thrusting. [3,5,8,9]
On internal examination (only with consent), clinicians may feel elevated resting tone, tenderness in the levator ani muscles, and limited descent when you try to bear down. [5,8,9] PFPT again has a central role. [5,8,9]
Deep Dyspareunia
Deep pain with penetration can be linked to several pelvic conditions, sometimes even when examination or ultrasound appears normal. [6,8,10,11]
 Book Appointment
Book Appointment When is Painful Sex a Red Flag?
Painful sex is very rarely an emergency, but there are situations where urgent assessment is important. [8,10] Knowing these can help you decide when to seek immediate support.
- Vulval Cancer/VIN Red Flags: New or changing vulval lesions, persistent ulceration, induration (hardness), non-healing fissures, unexplained bleeding, or progressive changes in vulval architecture. [8,10] These require urgent cancer pathway assessment.
- Systemic or Acute Illness Red Flags: Severe lower abdominal pain with fever, feeling very unwell, suspected tubo-ovarian abscess, or pelvic pain during pregnancy with bleeding or collapse. [10] These require emergency evaluation.
- Neurological Symptoms: New saddle anaesthesia (numbness around inner thighs/genitals) or new urinary retention/incontinence. [8,10]
- Trauma/Abuse: Pain associated with sexual trauma, coercion, or current abuse. [3,8] Services aim to respond in a trauma-informed way, offering safeguarding support.
If you are worried that any of these apply to you, it is usually safest to seek urgent medical advice—for example, via NHS 111, your GP, or emergency services.
5. What Happens at a Painful Sex Assessment?
A good assessment should feel collaborative, paced and consent-led, with space to pause or stop at any time. [3,8,9] Clinicians are encouraged to ask permission at each step. [3,8,9]
Trauma-Informed History
- When the pain began
- Location (entrance vs deep)
- Sensation (burning, raw, aching)
- Menstrual/obstetric history
- Past infections or PID
- Skin changes or rashes
- Bladder/bowel symptoms
- Emotional impact & fear [3,8]
Examination (With Consent)
- Visual inspection of vulva/perineum
- Cotton swab "mapping" for PVD
- Speculum offered (always optional)
- Internal exam for pelvic-floor tone
- Checking for deep tenderness [5,8–10]
Tests (When Needed)
Not everyone needs tests straight away. When they are used, they might include vaginal swabs, vulval biopsy for suspicious skin changes, patch testing for allergies, or pelvic transvaginal ultrasound (TVUS) to look for masses. [6,8,10,11]
Explaining Findings and Agreeing a Plan
Pain levels and examination findings do not always neatly match. [3,6,8] NICE endometriosis guidance explicitly cautions against dismissing symptoms purely because examination or ultrasound is normal. [6,11] A good consultation should validate your experience and outline a shared plan. [1,4,6,8,11,13,15]
6. Treatment Options Based on the Cause
Because painful sex is often multifactorial, treatment usually involves combining approaches. [1,3–6,8–10,15]
GSM-Related Dyspareunia
Guidelines recommend:
- Vaginal oestrogen as core treatment. [1,4,13,15]
- Moisturisers/lubricants as helpful adjuncts, not substitutes. [1,4,13]
- Discussing benefits, risks, and ongoing use.
PVD & Muscle Tension
First-line care includes:
- Multimodal PFPT (manual therapy, biofeedback). [5,8,9]
- Topical 5% lidocaine (as part of plan). [5]
- Psychosexual/CBT therapy for fear/avoidance. [3,5,8,9]
Deep Dyspareunia
NICE NG73 suggests:
- Hormonal suppression based on symptoms. [6,11]
- TVUS as first-line imaging. [6,11]
- Referral to specialist services for severe symptoms. [6,11]
Skin & Allergies
Treatment focuses on:
- Managing underlying dermatosis (e.g., steroids). [8,10]
- Gentle skincare & avoidance of irritants.
- Patch testing or biopsy where needed. [8,10]
Get Support Adjuncts, Procedures & Cautions
You may see therapies advertised online. Some have limited evidence; others are flagged as potentially harmful. [5,7,8,14]
Energy-Based Vaginal Lasers & Radiofrequency
An FDA safety communication warns that safety and effectiveness for these indications have not been established, and reports of burns, scarring, and worsened dyspareunia exist. [7,14] Expert opinion is that these devices should not be marketed as routine treatment. [7,8,14]
Other Modalities
Evidence for TENS, LLLT, shockwave and EMG biofeedback is mixed/low-quality and they cannot be recommended as stand-alone treatments. [5,8,14] Complementary therapies (Acupuncture, Ayurveda) have limited evidence but may be supportive adjuncts. [8]
Common Myths
- "Moisturisers are equal to oestrogen for GSM": Helpful, but not equivalent for pain relief. [1,4,13,15]
- "Lidocaine works as well as PFPT": RCT evidence shows PFPT is superior. [5]
- "Normal exam means no endometriosis": NICE says do not exclude based on normal exam. [6,11]
8. Getting the Right Support and Specialist Care
UK and international guidance recommends multidisciplinary care for complex pain. [3,5,8–10,12] This might include gynaecology, dermatology, pelvic-health physiotherapy, psychosexual therapy and pain medicine. [8,12]
You might be referred to:
- Specialist vulval clinic (complex dermatoses, VIN, vestibulodynia)
- Endometriosis/pelvic pain service (deep dyspareunia)
- Urogynaecology/urology (bladder pain)
- Pelvic-health physiotherapy
- Psychosexual therapy [3,5,8–12]
9. Living with Painful Sex
Living with painful sex is not just a medical issue; it can touch every part of your life. [2,3,5,8] Trauma-informed and psychosexual approaches emphasise:
Self-care might include paced experimentation with vaginal dilators (ideally under PFPT guidance), using lubricants generously, scheduling rest around flares, and connecting with support groups. [5,8]
10. Questions You Might Ask Your Clinician
You are entitled to clear explanations and shared decision-making. [1,3–6,8–11,15]
- Based on my story and exam, what do you think are the main possible causes?
- Does my pain sound mostly "entry-related", "deep", or a mix?
- Are there any red flags you are concerned about?
- What tests do you recommend, and what would they change about management?
- How might my menopause status or medications be contributing?
- Could pelvic-floor physiotherapy help, and how do I access it?
- What are the likely benefits/uncertainties of vaginal oestrogen for me?
- When would you consider referring me to a specialist clinic?
11. Key Research Gaps
Even though painful sex is common, important gaps remain. [5,7,8,14] Guidelines highlight the need for validated dyspareunia-specific outcome measures, comparative-effectiveness trials (e.g., PFPT vs meds), long-term safety data for procedures/lasers, and equity/access studies. [2,5,7,8,12,14]
For you, this means treatments may need to be tailored based on best-available evidence and values. [5,7,8,14]
12. Key Statistics at a Glance
13. About this guide and the evidence
This article is based on a merged, externally validated research summary created by comparing multiple base documents against current UK and international guidance. [1–15] The process prioritised UK guidelines (NICE, BSSVD, BMS), consensus terminology, RCT evidence, and IUSTI guidance. [1,4,5,8,10]
14. Medically reviewed by
Medically reviewed by the clinical team at The Women’s Health Clinic, using current guidance from NICE, BMS, BSSVD, ISSVD/ISSWSH/IPPS and IUSTI. [1–11,15]
15. References & Evidence
16. Frequently Asked Questions
What is dyspareunia (pain with sex) and how is it classified?
Dyspareunia means persistent or recurrent genital pain with sexual activity. Clinicians usually separate entry (superficial) pain from deep pain, because causes and care pathways differ. [2,3]
Read more in our FAQ: What is dyspareunia and how is it classified? →What is the difference between superficial and deep dyspareunia?
Superficial dyspareunia is pain at or just inside the vaginal opening, while deep dyspareunia is felt higher in the pelvis during penetration. This distinction helps your clinician think about likely causes (for example GSM, vulval pain, pelvic-floor tension, or deep conditions such as endometriosis) and plan next steps. [3,4,6]
Read more in our FAQ: What is the difference between superficial and deep dyspareunia? →What are the most common causes of painful sex in women?
Painful sex is usually multifactorial. Common contributors include genitourinary syndrome of the menopause (GSM), provoked vestibulodynia (PVD), pelvic-floor muscle overactivity, vulval dermatoses (such as lichen sclerosus), infections, postpartum scarring, and deeper causes such as endometriosis/adenomyosis. [3,4,6,8,10,11]
Read more in our FAQ: What are the most common causes of painful sex in women? →What medical conditions cause painful sex in women?
Medical conditions that can drive dyspareunia include GSM, vulvodynia/PVD, pelvic-floor myalgia, vulval skin conditions (e.g. lichen sclerosus), recurrent infections, postpartum perineal trauma, endometriosis/adenomyosis, PID, ovarian cysts and bladder pain syndrome (IC/BPS). [3,4,6,8,10,11]
Read more in our FAQ: What medical conditions cause painful sex in women? →How common is painful sex after childbirth or menopause?
A large UK study (Natsal-3) found that about 7.5% of sexually active women reported painful sex in the previous year. [2] Painful sex is often reported around childbirth (due to trauma or muscle tension) and around menopause (due to GSM and dryness). [4,8]
Read more in our FAQ: How common is painful sex after childbirth or menopause? →Endometriosis/adenomyosis and deep dyspareunia — what should I know?
Endometriosis and adenomyosis can cause deep pelvic pain with penetration. NICE guidance stresses that endometriosis should not be excluded just because pelvic examination or ultrasound are normal, and recommends considering hormonal suppression and referral when symptoms affect daily life. [6,11]
Read more in our FAQ: Endometriosis/adenomyosis and deep dyspareunia — what should I know? →What are the long-term effects of chronic dyspareunia?
Chronic dyspareunia can contribute to ongoing pelvic pain, avoidance of intimacy, reduced sexual satisfaction and distress. [2,3] Data show strong associations with relationship difficulties and worse mental health scores. [2,8]
Read more in our FAQ: What are the long-term effects of chronic dyspareunia? →Can dyspareunia return after successful treatment?
Yes. Symptoms can flare again if the underlying condition changes or if treatments (like vaginal oestrogen) are stopped. [4,13] Ongoing review and self-care strategies are often important. [3,4,6,8]
Read more in our FAQ: Can dyspareunia return after successful treatment? →Is vaginal atrophy painful during intercourse?
Yes. GSM (which includes vaginal atrophy) causes dryness, burning, tissue fragility and both superficial and deep pain. [4,13,15] NICE and BMS support offering vaginal oestrogen with ongoing use when helpful. [4,13,15]
Read more in our FAQ: Is vaginal atrophy painful during intercourse? →What causes vaginal dryness in 20s and 30s?
Vaginal dryness can occur at any age. In younger women, contributors include lactation, premature ovarian insufficiency, anti-oestrogen therapies, infections or skin conditions. [4,10,13]
Read more in our FAQ: What causes vaginal dryness in 20s and 30s? →Does vaginal dryness start before periods stop?
Yes. In the perimenopause, hormone levels fluctuate, and some people notice dryness or pain before their final period. [1,4,13,15]
Read more in our FAQ: Does vaginal dryness start before periods stop? →When should I see a doctor for vaginal dryness?
Seek advice if dryness is persistent, affects comfort/sex, or is associated with bleeding or skin changes. [4,10,13]
Read more in our FAQ: When should I see a doctor for vaginal dryness? →What is the difference between vaginal atrophy and vaginal dryness?
Vaginal dryness is a symptom. Vaginal atrophy/GSM is a diagnosis where oestrogen-responsive tissues become thinner and inflamed, causing dryness, urinary symptoms and pain. [4,13,15]
Read more in our FAQ: What is the difference between vaginal atrophy and vaginal dryness? →Medically reviewed by the clinical team at The Women’s Health Clinic. Educational only. Not medical advice.
Sources: NICE, BMS, BSSVD, ISSVD/ISSWSH/IPPS and IUSTI.