Content approved by: Dr Farzana Khan, MD, MRCGP, DFFP — Specialist in vaginal health with 20+ years’ medical experience across dermatology and gynaecology. Care is balanced, evidence-aware, and patient-centred.
Dr Farzana Khan qualified as an MD from the University of Copenhagen in 2003. She has worked in dermatology and obstetrics & gynaecology across the North of England and completed her MRCGP (CCT, 2013) and the Diploma of the Faculty of Sexual & Reproductive Health (2013).
Her clinical focus is vaginal health—including dryness/GSM, sexual function concerns, lichen sclerosus, and comfort or volume changes. She explains conservative and medical options first, then discusses regenerative or aesthetic procedures where appropriate.
Dr Farzana is a key opinion leader on women’s intimate health and been featured in the press including the daily mail and on BBC radio. Dr Farzana also trains clinicians as a Trainer with Neauvia, NuV Laser, Asclepion Juliet Laser, and RegenLab. Ongoing CPD includes IMCAS, CCR, ACE and expert training in intimate fillers, PRP and polynucleotides.
Authored and medically reviewed by Dr Farzana Khan. Last updated: 1 November 2025.
Clinical Practice Guideline: Assessment and Management of Dyspareunia
Key Takeaways
- Multifactorial Nature: Dyspareunia requires a biopsychosocial assessment, acknowledging the interplay of physical pathology, psychological impact, and relational dynamics.
- Accurate Classification: Distinguishing between superficial (entry) and deep pain is the critical first step in narrowing the differential diagnosis.
- Evidence-Based First Line: Conservative therapies, including local oestrogen, specialist physiotherapy, and psychosexual support, are the gold standard for initial management.
- Procedural Caution: Energy-based devices and injectables are second-line or adjunct therapies and require strict adherence to safety protocols and informed consent.
Table of Contents
1.0 Introduction to Dyspareunia
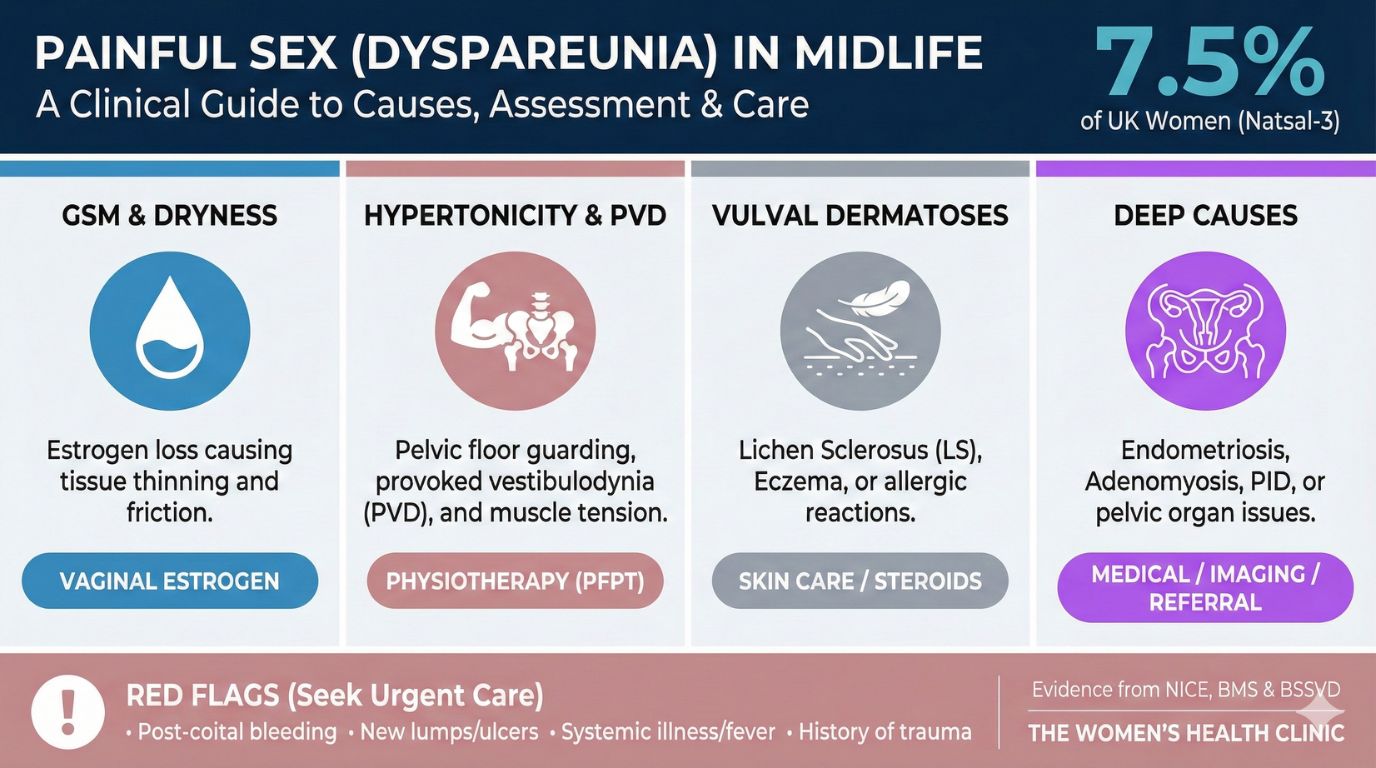
Dyspareunia is defined as persistent or recurrent genital pain associated with sexual intercourse. It is a common and distressing condition, with the Natsal-3 study reporting a prevalence of 7.5% among sexually active women in the UK. The strategic purpose of this guideline is to provide healthcare professionals with a structured, evidence-based framework for the assessment and management of this multifactorial condition. It aims to move clinical practice beyond simplistic diagnoses towards a comprehensive biopsychosocial model that acknowledges the interplay between physical pathology, psychological impact, and relational dynamics.
This document synthesizes current clinical best practices from authoritative bodies including the National Institute for Health and Care Excellence (NICE) and the Royal College of Obstetricians and Gynaecologists (RCOG). The critical first step in successfully managing dyspareunia is a thorough, empathetic, and structured clinical assessment.
1.2 Clinical Classification of Dyspareunia
Dyspareunia is classified clinically by its location and onset to help narrow the differential diagnosis and guide subsequent investigation.
Classification by Location
- Superficial (Entry): Pain localised to the vulva or vaginal entrance (introitus). Occurs immediately upon touch; often described as burning, stinging, or "raw paper cut." Points to skin, nerve, or pelvic floor issues.
- Deep Dyspareunia: Pain experienced higher in the vagina or deep in the pelvic cavity during thrusting. Described as deep aching, "bruised," or "collision" pain. Suggests irritation of uterus, ovaries, or bladder.
Classification by Onset
- Primary: Pain present since the first attempt at penetration. May suggest congenital factors or early vaginismus.
- Secondary: Pain develops after a period of pain-free activity. More common; often follows childbirth, surgery, menopause, or conditions like endometriosis.
 Book Appointment
Book Appointment 2.0 Clinical Assessment and Triage
The initial consultation is the cornerstone of effective management. A detailed clinical history provides up to 80% of the diagnostic clues, often making it more valuable than the physical examination. The assessment must follow a Bio-Psycho-Social model, acknowledging the intricate interplay between physical pathology, psychological impact, and relational context.
2.2 Structured History Taking: The Pain Map
To build a comprehensive understanding, history taking should be structured to create a detailed "Pain Map":
- Location: "Is the pain felt at the entrance ('paper cut') or deep inside ('bruised')? Can you point with one finger?"
- Timing: "Does it occur immediately on contact or develop as a dull ache afterwards?"
- Quality: "Is it 'burning' (nerve/skin) or like 'hitting a wall' (muscle spasm)?"
- Context: Menstrual cycle links, contraception use, and obstetric history.
2.3 The Trauma-Informed Physical Examination
A physical examination is a valuable diagnostic tool but is not always mandatory on the first visit, especially in cases of severe vaginismus. When performed, it must be patient-controlled (using "Traffic Light" signals). Key steps include external inspection for Lichen Sclerosus, the "Q-Tip Test" for nerve hypersensitivity (allodynia), and a single-digit muscle check for hypertonicity.
2.4 Diagnostic Investigations
| Test / Referral | Indication | Key Clinical Insights |
|---|---|---|
| Vaginal Swabs & pH | Abnormal discharge/odour. | pH <3.5: Cytolytic Vaginosis. pH >4.5: Bacterial Vaginosis (BV). |
| STI Screening | New partner or PID symptoms. | Respect window periods (e.g., 2 weeks for Chlamydia). |
| Transvaginal Ultrasound | Deep pelvic pain or mass. | First-line for deep pain. Normal scan does not rule out endometriosis. |
2.5 Identifying Red-Flag Symptoms
Immediate A&E / 999
- Hemorrhage: Soaking 1 pad/hour for 2 hours.
- "Thunderclap" Pain: Sudden, severe, +/- vomiting (Ovarian Torsion).
- Cauda Equina Signs: Saddle anaesthesia or loss of bladder/bowel control.
Urgent GP Review (2WW)
- Post-Menopausal Bleeding: Any bleeding after 12 months amenorrhea.
- New "IBS" Over 50: Unexplained bowel changes or bloating (Ovarian pathology check).
3.0 Differential Diagnoses for Introital (Superficial) Dyspareunia
Pain localised to the vaginal entrance is multifactorial. This section evaluates primary causes to move beyond a label of 'painful sex' to specific drivers.
3.1 Hormonal and Atrophic Changes
Low oestrogen (menopause, breastfeeding, hormonal contraceptives) leads to Genitourinary Syndrome of Menopause (GSM), causing thin, dry tissue. The combined pill can also cause the "SHBG trap," increasing Sex Hormone-Binding Globulin and lowering free testosterone, leading to vestibulodynia.
Neuropathic & Muscular
Provoked Vestibulodynia (PVD): Nerve hypersensitivity (allodynia) at the vestibule. Sharp/burning pain. Diagnosed via Q-tip test.
Vaginismus: Involuntary guarding reflex/spasm of pelvic floor muscles. Distinct from hypertonicity (chronic tightness/trigger points) which requires "Down-Training."
Dermatological & Infectious
Lichen Sclerosus: White, fragile "parchment" patches that tear easily.
Cytolytic Vaginosis (CV): Overgrowth of "good" bacteria causing acidic burning (pH <3.5). Often confused with Thrush but antifungals make it worse.
Struggling with unexplained pain?
Get Support4.0 Differential Diagnoses for Deep Dyspareunia
Deep dyspareunia is typically mechanical, termed "collision dyspareunia," felt high in the vagina. It often suggests structural pathology.
[Image of endometriosis vs adenomyosis uterus comparison]4.1 Endometriosis and Adenomyosis
These are "twin" but distinct conditions. Endometriosis is tissue outside the uterus (ovaries, Pouch of Douglas), causing sharp, stabbing pain. Adenomyosis is tissue within the uterine muscle wall, causing a boggy, tender uterus and deep "bruised" pain. Note: A normal ultrasound does not exclude endometriosis.
4.2 Other Pelvic Pathology
- Ovarian Cysts/Endometriomas: "Chocolate cysts" can cause unilateral pain.
- Pelvic Inflammatory Disease (PID): Infection causing adhesions and organ restriction.
- Musculoskeletal: Myofascial trigger points in the Obturator Internus can refer pain to the hip or deep pelvis.
- Pudendal Neuralgia: Nerve pain in the "saddle area," worsened by sitting ("Toilet Seat Sign" offers relief).
5.0 Evidence-Based Management: Conservative Therapies
Conservative, non-invasive therapies are the first-line approach, often combined for a synergistic effect.
Core Modalities
- Hormonal Therapies: Local vaginal oestrogen is the gold standard for GSM. Vaginal DHEA (Prasterone) is an option for dryness plus loss of sensation.
- Specialist Pelvic Physiotherapy: Focuses on "Down-Training" (relaxing) hypertonic muscles, internal myofascial release, and desensitisation using dilators. Note: True muscle change takes 8-12 weeks.
5.3 Medication Review
Common medications can contribute to dyspareunia. A review is essential.
| Class | Mechanism | Strategy |
|---|---|---|
| SSRIs | "Sensation blocker" (delayed orgasm). | Switch to Mirtazapine or Bupropion. |
| Hormonal Contraceptives | Increases SHBG, lowers testosterone. | Switch to non-hormonal IUD or transdermal patch/ring. |
6.0 Procedural and Regenerative Therapies
Procedural therapies are adjuncts, not replacements for standard care. Energy-based devices (Laser/RF) are reserved for those who fail local oestrogen, per NICE guidance.
6.2 Regenerative Injectables
| Treatment | Mechanism | Best For |
|---|---|---|
| PRP (O-Shot) | Growth factors stimulate neuro/angiogenesis. | Sensation loss, Lichen Sclerosus. |
| Polynucleotides | Signals cellular repair and hydration. | Severe atrophy ("paper thin" skin). |
| HA Fillers | Volume and structural cushion. | Frictional enhancement, deflated labia. |
Expert Care for Complex Cases
We offer a multidisciplinary approach combining medical, physical, and psychological therapies.
7.0 Long-Term Management and Patient Care
Adherence to the "Montgomery Standard" for consent is vital, ensuring patients understand material risks. A cooling-off period is mandatory for elective procedures.
7.2 Aftercare and Recovery
| Procedure | Abstinence | Rationale |
|---|---|---|
| Vaginal Laser | 5–7 Days | Allow microscopic channels to heal; prevent infection. |
| PRP (O-Shot) | 24 Hours | Seal entry points. NSAID Ban: Avoid anti-inflammatories for 5-7 days pre/post treatment. |
Disclaimer: This content is for informational purposes only and does not constitute medical advice. Consult a healthcare professional for diagnosis and treatment.