
Clinical Review & Disclaimer
- Verified Content: Approved by the Women’s Health Clinic Clinical Team.
- Educational Use: This is not a substitute for professional medical advice, diagnosis, or treatment.
- Clinical Assessment: Individual suitability is determined by a clinician; results may vary.
- MEDICAL EMERGENCY: If you are experiencing a medical emergency, call 911 immediately.
About the Author

Lichen Sclerosus Treatment UK: Vulval LS Support with Laser, RF, PRP & Polynucleotides
Assessment-led care across our CQC-regulated UK clinics
Lichen sclerosus (LS) can be physically uncomfortable and emotionally exhausting. Many women in the UK describe the same quiet loop: itching that won’t settle, soreness that flares without warning, fragile skin that tears easily, and intimacy that starts to feel stressful instead of safe.
If that’s you, you’re not alone—and you’re not “overreacting.”
Lichen sclerosus is a long-term inflammatory skin condition that most commonly affects the vulval area in women. It cannot be cured, but it can often be managed well with the right treatment plan and consistent follow-up. (nhs.uk)
At The Women’s Health Clinic, we support women across the UK with vulval lichen sclerosus using a clinically governed, multi-layer approach. That means:
- We discuss and optimise standard first-line lichen sclerosus care (usually potent prescription steroid ointment plus barrier care), in line with recognised UK guidance. (British Association of Dermatologists)
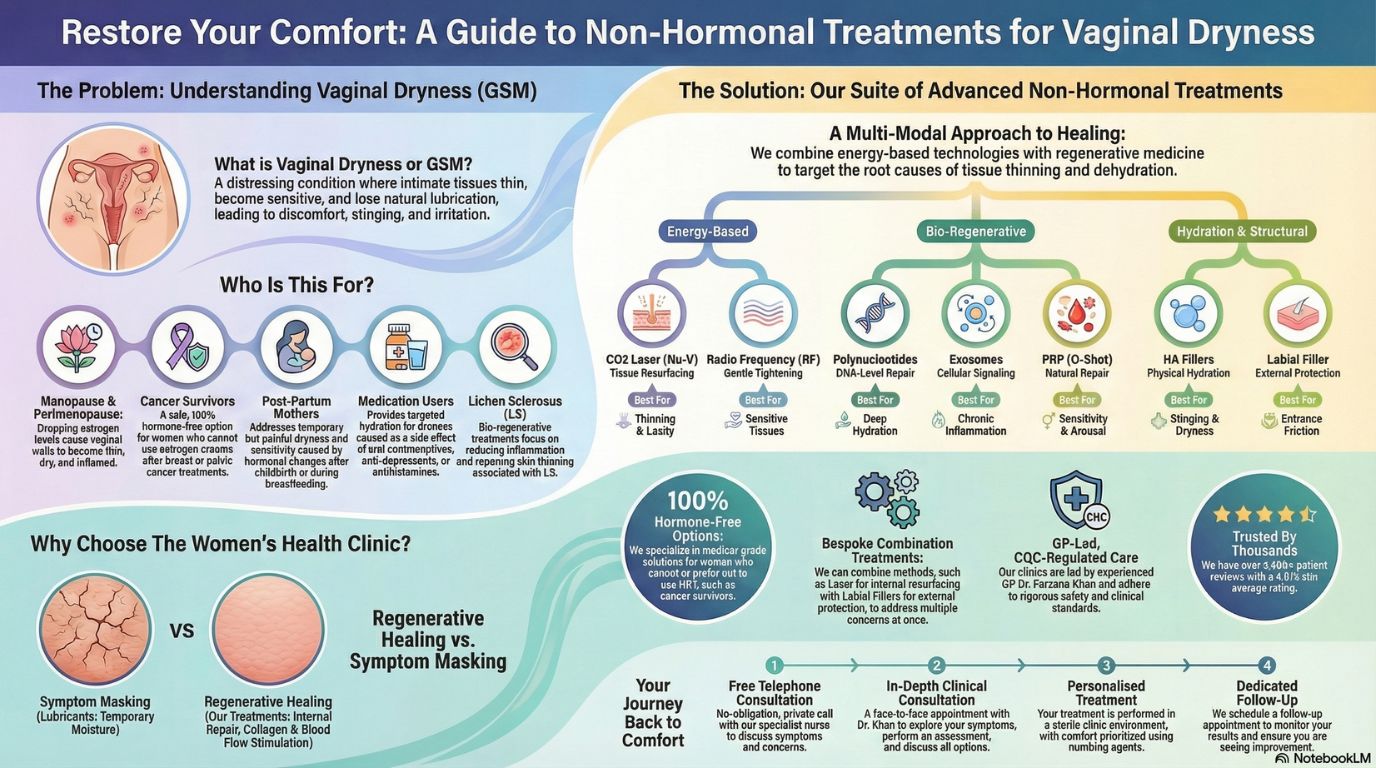
- Where appropriate, we may consider adjunct regenerative options to support comfort and tissue quality, including: laser, radiofrequency (RF), PRP, and polynucleotides.
Important note: This page provides educational information only. Results vary and no treatment is guaranteed. LS requires medical assessment, ongoing monitoring, and a plan tailored to your symptoms and examination findings.
Why Women Choose Our Lichen Sclerosus Clinic
- CQC-regulated medical clinics across the UK
- GP-led women’s intimate health care (assessment first)
- Adjunct regenerative options explored carefully, where appropriate
- Evidence-informed counselling (benefits, limits, uncertainty)
- Clinics nationwide – London (Harley Street), Canary Wharf, Leicester, Leeds, Birmingham, Harrogate, Bristol, Exeter, Manchester
Practitioner-led vulval LS care
Treatments delivered by Dr Farzana Khan (GP & Women’s Health Specialist).
Medical oversight
Compliance led by Dr Kamaljit Singh (Clinical Oversight) and Katy Pitt Allen (Clinical Director).
Treatment Summary
What Is Lichen Sclerosus?
Lichen sclerosus (also called LS or vulval lichen sclerosus) is a chronic inflammatory skin condition that most often affects the vulval area in women. Vulval lichen sclerosus may cause:
- Vulval itching (often worse at night)
- Soreness or burning
- Tiny cracks (fissures) and easy tearing
- White, shiny patches or texture changes
- Discomfort with sex, wiping, or sitting
- Scarring or tightening over time if not controlled
Because lichen sclerosus can change the skin’s structure, it’s not just “dryness” or “thrush.” Vulval LS needs the right diagnosis and a long-term management plan. (Wirral University Hospital)
The Non-Negotiable Foundation
Most recognised UK guidance describes strong prescription steroid ointment (commonly clobetasol propionate 0.05%) as the mainstay of lichen sclerosus treatment, typically started with an intensive regimen and then reduced to maintenance. (British Association of Dermatologists)
A commonly described regimen is: daily for a period (often 1 month), then alternate days, then twice weekly—followed by an individualised maintenance schedule. (British Association of Dermatologists)
Maintenance treatment (often twice weekly) is commonly recommended for many patients to reduce flare-ups and protect vulval tissue long-term. (BSSVD)
Why Monitoring Matters
Lichen sclerosus is associated with a small but real increased risk of vulval cancer, so ongoing monitoring and self-examination are important parts of LS care. (British Association of Dermatologists)
Clinically governed, long-term LS care
Vulval lichen sclerosus is a long-term condition. The goal is structured management—control, comfort, and careful follow-up—so you feel supported, not stuck in cycles.
Get Clinical SupportWho Is This For?
Adjunct regenerative options may be considered for carefully selected women—especially when standard LS care is optimised but comfort, fragility, or flare patterns remain difficult.
Confirmed or suspected LS
Have a confirmed (or strongly suspected) diagnosis of vulval lichen sclerosus and want specialist support.
Persistent symptoms
Are using standard LS care but still struggle with comfort, fragility, or recurrent flare patterns.
Friction sensitivity
Experience soreness and friction sensitivity despite careful emollient and barrier care.
Tightness or scarring
Have symptoms of scarring/tightness that need specialist evaluation and a personalised plan.
Clinician-led support
Want realistic expectations, careful counselling, and follow-up—not device-first care.
Monitoring-focused
Want an LS plan that includes monitoring and clear guidance on when to seek urgent review.
Who these treatments may not be suitable for
- Active vulval/urinary/vaginal infection
- Undiagnosed vulval lesions that need assessment or biopsy first
- Pregnancy
- Certain immune/bleeding disorders (individual assessment)
- Known allergies relevant to specific injectables (discussed in Safety)
Comfort-led care, without hype
We prioritise clear counselling: what’s standard, what’s adjunct, what the evidence says, and what’s realistically possible for you.
Why Women Explore Treatment
Standard LS treatment can be very effective for inflammation control. But many women still want support for fragility, friction sensitivity, and quality-of-life confidence—especially around daily comfort and intimacy.
Symptom control vs tissue support
- Fragile, tear-prone skin and fissures
- Soreness and friction sensitivity
- Intimacy feeling stressful rather than safe
- Confidence and comfort day-to-day
Think of it like caring for a delicate fabric: you control the “irritation” first (inflammation), then you may explore ways to support how the fabric feels and holds up over time (tissue comfort).
Assessment-led, honest, and long-term
We start by understanding your LS pattern: symptoms, triggers, exam findings, current regimen, and whether anything needs urgent review first. Adjunct options are only discussed where they make clinical sense—and always with realistic expectations.
A transparent note on evidence (important)
It’s easy to find strong marketing claims online about lasers, RF, PRP and “regenerative” options for lichen sclerosus. The reality is more nuanced: evidence exists, but quality and consistency vary by method and study.
- Laser: some studies show improvement for some patients; evidence is mixed and evolving. (OUP Academic)
- RF: emerging literature including small studies/pilots. (PMC)
- PRP: trials and reviews exist, but conclusions remain cautious due to heterogeneity. (PMC)
- Polynucleotides: used as biostimulatory agents in other contexts; LS-specific evidence is limited and discussed case-by-case. (ScienceDirect)
Our approach to LS treatment
- Detailed assessment first (symptoms, triggers, exam findings, current regimen)
- Screening for red flags and investigation/referral when needed
- Optimising standard care first; adjunct options only if appropriate
- Realistic counselling on benefits, limitations, and uncertainty
How It Works
Our process is divided into two parts: the adjunct methods we may discuss (where appropriate) and the clinical journey we guide you through.
Part A: Methods We May Discuss
Laser (Adjunct)
What happens: Controlled laser energy is delivered to targeted tissue as part of a structured clinical protocol.
Why it may be used: Intended to stimulate a tissue response that may support symptoms and tissue quality in selected vulval LS cases (evidence is mixed and evolving). (OUP Academic)
What it feels like: Warmth and tingling; comfort measures used.
Downtime: Typically short pelvic rest (often ~5 days), plus tailored aftercare.
Radiofrequency (RF)
What happens: Controlled warmth delivered to deeper tissue layers without breaking the skin surface.
Why it may be used: Often positioned as a gentler option; literature is emerging. (PMC)
What it feels like: Gentle warmth; usually very manageable.
Downtime: Usually minimal; most women return to normal activities same day.
PRP (Adjunct)
What happens: Blood is taken, platelets are concentrated, and PRP is applied/injected using a medical protocol.
Why it may be used: Studied in LS for symptom/tissue support; overall conclusions remain cautious due to limited and heterogeneous evidence. (PMC)
What it feels like: Brief blood draw + injections with numbing; 24–48h tenderness possible.
Downtime: Usually minimal; tailored aftercare provided.
Polynucleotides
What happens: Targeted injections to support tissue hydration/biostimulation goals.
Why it may be used: Used in other regenerative contexts; LS-specific evidence is limited and discussed transparently case-by-case. (ScienceDirect)
What it feels like: Numbing used; mild pressure rather than pain.
Downtime: Usually minimal.
Part B: Your 6-Step Patient Journey
Step 1: Free Telephone Consultation
Confidential nurse call: discuss your LS symptoms, goals, and next steps. No pressure.
Step 2: Book Your Appointment
Pre-visit questionnaires so your consultation time is focused on your symptoms and priorities.
Step 3: In-Person Consultation
This is where the plan becomes clear. During this appointment we:
Assess: symptom pattern, current regimen, triggers, skin changes (with your consent), and whether anything needs urgent review.
Discuss: optimising standard care, realistic goals, and whether any adjunct options are appropriate for you.
Step 4: Treatment (If Appropriate)
If you choose to proceed and provide informed consent, treatment is delivered with comfort, dignity, and clear aftercare.
Timing: most procedures take 30–60 minutes depending on method and treatment area.
Step 5: Feedback
We check how you felt about the experience, what changed, and what you need next.
Step 6: Follow-Up
We reassess symptoms and tissue response, adjust the plan if needed, and discuss maintenance only if it makes sense for you.
Ongoing support: if you have questions between appointments, our team is available to help.
About Our Clinical Team
Expert vulval health care requires medical expertise, careful follow-up, and genuinely compassionate support.
Dr. Farzana Khan
BSc (Hons), MD, DFFP, MRCGP
Dr. Farzana Khan is a highly experienced GP with a special interest in vulval and vaginal health, bringing over 20 years of medical expertise across dermatology, obstetrics, and gynaecology.
- Qualifications: MD (University of Copenhagen), MRCGP, and Diploma of the Faculty of Sexual & Reproductive Health.
- Clinical Focus: Vulval dermatoses including lichen sclerosus, GSM/vaginal dryness, sexual discomfort, and broader intimate health concerns.
- Approach to Care: Dr. Khan believes in “listening first.” She ensures standard and conservative options are thoroughly explored and optimised before discussing adjunct procedures.
- Expert Training: Dr. Khan is a Key Opinion Leader (KOL) and trainer for leading medical technologies, including Neauvia, Asclepion Laser, and RegenLab.
You’ll receive clear, balanced counselling on benefits, limitations, and risks—so you can decide with realistic expectations and no pressure.
Our Clinical Management & Compliance Team

Katy Pitt Allen
Clinical Director (RN, BMS)
With over a decade of nursing excellence in oncology, gynaecology, and palliative care, Katy ensures rigorous clinical standards and compassionate care.

Dr. Kamaljit Singh
Clinical Oversight (MBChB)
Dr. Singh provides medical oversight, ensuring robust safety protocols, governance, and consistent standards across clinics.

Jill Crowe
Director of Relationships
Jill coordinates a seamless patient journey—so you feel supported from first call through follow-up.
"Our specialist vulval health treatments are delivered across our CQC-regulated clinics in London (Harley Street), Canary Wharf, Leicester, Leeds, Birmingham, Harrogate, Bristol, Exeter, and Manchester."
Authored and medically reviewed by Dr. Farzana Khan. Last updated: December 2025.
Transparent Pricing
Lichen sclerosus care is individual. Pricing depends on symptom severity, distribution of vulval LS, whether you’re in flare or stable phase, and whether an adjunct course is recommended.
PRP (Adjunct)
Laser Course (If Recommended)
Course pricing is designed for women advised a structured protocol. Suitability is confirmed after clinical assessment.
- Clinical time and consumables
- Aftercare guidance
- Planned follow-up appointments
RF & Polynucleotides
Protocols can vary depending on treatment area and goals, so final pricing is confirmed after assessment.
RF: £699 per session (course plan if recommended)
Polynucleotides: £699 per treatment (course plan if recommended)
What’s included: practitioner time, clinical consumables, aftercare guidance, and planned follow-up.
Concerns & Safety
Red flags: when LS needs urgent review first
- Persistent sore/ulcer (especially > 4 weeks)
- New lump, thickening, or hardening (induration)
- New crusted or non-healing area
These are common triggers for urgent assessment in LS follow-up guidance. (BSSVD)
General contraindications (often include)
- Pregnancy
- Active infection in the vulval area
- Undiagnosed bleeding
- Unassessed suspicious vulval lesions
Method-specific considerations
Laser / RF: temporary sensitivity, swelling, or irritation can occur; short pelvic rest is often advised after laser; implanted electronic devices may be relevant for RF suitability (assessed clinically).
PRP: uses your own blood components (low allergy risk), but may not be suitable for some blood disorders or active systemic infection (assessed individually).
Polynucleotides: often derived from purified fish DNA sources—please disclose fish allergy so we can advise safely. (ScienceDirect)
Reassuring but honest: lichen sclerosus has a small increased cancer risk (often described as < 5%), which is why monitoring matters. Good symptom control may reduce risk. (British Association of Dermatologists)
Frequently Asked Questions
Can lichen sclerosus be cured?
What is first-line treatment for vulval lichen sclerosus?
Are laser, RF, PRP or polynucleotides a replacement for steroid ointment?
What symptoms should I watch for that may need urgent review?
Is there a cancer risk with lichen sclerosus?
How many sessions will I need?
Will treatment hurt?
Will results be permanent?
You Don’t Have to Battle Lichen Sclerosus Alone
If you’ve been coping quietly with vulval lichen sclerosus—itching, burning, tearing, and anxiety about intimacy—you deserve a plan that feels structured, safe, and genuinely supportive.
What happens next is entirely up to you:
- Start with a free, no-obligation telephone consultation about lichen sclerosus
- Book an in-person assessment for diagnosis confirmation and bespoke planning
- Proceed only if it feels right for you
Start your journey to comfort today.
All treatments are delivered in CQC-regulated clinics with full medical oversight. Individual results vary. A consultation is required to assess suitability.
This page is for educational purposes only and does not constitute medical advice. Results vary. Not a cure.
The Women’s Health Clinic – Specialist Vulval Health Support Across the UK
CQC-regulated | GP-led | Evidence-informed | Nationwide locations