
Content approved by: Dr Farzana Khan, MD, MRCGP, DFFP — Specialist in vaginal health with 20+ years’ medical experience across dermatology and gynaecology. Care is balanced, evidence-aware, and patient-centred.
Dr Farzana Khan qualified as an MD from the University of Copenhagen in 2003. She has worked in dermatology and obstetrics & gynaecology across the North of England and completed her MRCGP (CCT, 2013) and the Diploma of the Faculty of Sexual & Reproductive Health (2013).
Her clinical focus is vaginal health—including dryness/GSM, sexual function concerns, lichen sclerosus, and comfort or volume changes. She explains conservative and medical options first, then discusses regenerative or aesthetic procedures where appropriate.
Dr Farzana is a key opinion leader on women’s intimate health and been featured in the press including the daily mail and on BBC radio. Dr Farzana also trains clinicians as a Trainer with Neauvia, NuV Laser, Asclepion Juliet Laser, and RegenLab. Ongoing CPD includes IMCAS, CCR, ACE and expert training in intimate fillers, PRP and polynucleotides.
Authored and medically reviewed by Dr Farzana Khan. Last updated: 1 November 2025.
Briefing on Pelvic Pain, Sexual Function, and Treatment Modalities
Executive Summary
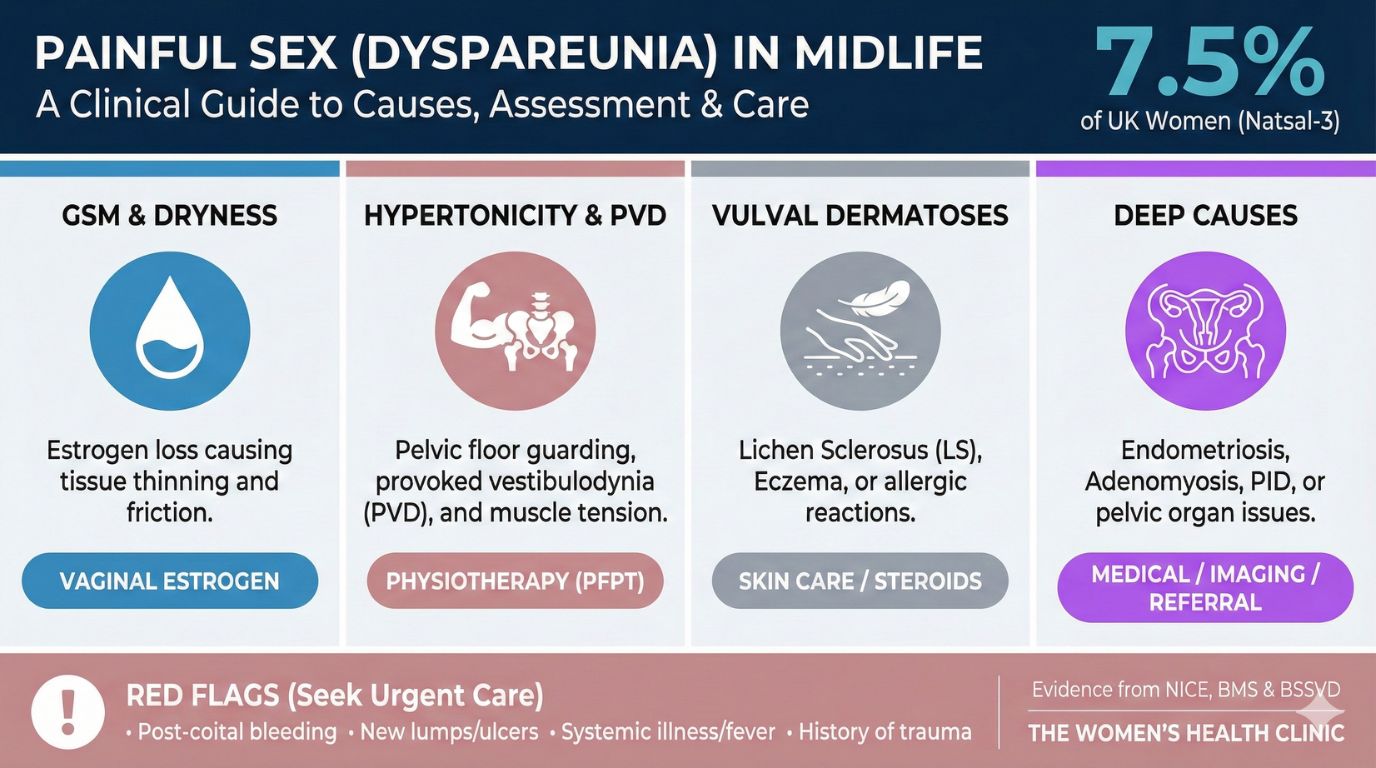
- Not Just Psychological: Dyspareunia is a multifactorial medical condition requiring clinical mapping of superficial vs. deep pain.
- Root Causes: Drivers range from hormonal (GSM) and musculoskeletal (hypertonicity) to structural (endometriosis) and medication side effects.
- Evidence-First: Foundational care (hormones, physio, therapy) is the gold standard. Regenerative procedures (Laser, PRP) are adjunctive options requiring robust consent.
- Safety Protocol: Patient safety relies on trauma-informed exams, certified devices (UKCA/CE), and adherence to biological healing timelines.
Table of Contents
1.0 The Multifaceted Nature of Painful Sex (Dyspareunia)
Dyspareunia is persistent genital pain occurring before, during, or after sexual activity. Accurate diagnosis relies on classifying the location and onset of the pain.
By Location
- Superficial (Entry): Pain at the vulva/introitus on initial touch. Described as burning, stinging, or tearing.
- Deep Dyspareunia: Pain deep in the pelvis during thrusting. Described as aching, cramping, or "collision."
By Onset
- Primary: Pain present since the first attempt at penetration.
- Secondary: Pain developed after a period of comfortable function.
2.0 Key Causes and Contributing Factors
Hormonal & Musculoskeletal
Genitourinary Syndrome of Menopause (GSM): Low estrogen causes tissue atrophy (thinning/dryness). Chronic and progressive without treatment.
Pelvic Floor Hypertonicity: Chronic muscle guarding or spasm. Trigger points can refer pain to hips or bladder.
[Image of pelvic floor muscles and obturator internus]Neuropathic & Structural
Provoked Vestibulodynia (PVD): Nerve hypersensitivity at the entrance. Sharp pain on light touch; skin often looks normal.
Endometriosis & Adenomyosis: Ectopic tissue growth causing cyclical deep pain and dyschezia (painful bowel movements). Note: "Normal" ultrasound does not rule these out.
[Image of endometriosis vs adenomyosis uterus comparison]Medication Impact
- SSRIs: Can blunt genital sensation and delay orgasm ("Genital Anaesthesia").
- Hormonal Contraceptives: Can raise SHBG, lowering free testosterone and thinning vestibular tissue.
- Antihistamines/Roaccutane: Systemic drying effect on mucous membranes.
 Book Assessment
Book Assessment 3.0 Diagnostic Pathways and Clinical Assessment
Assessment relies on 80% history taking ("Pain Mapping") and a consent-based physical exam.
| Technique | Key Findings |
|---|---|
| Q-Tip Test | Sharp pain at 5 & 7 o'clock indicates Provoked Vestibulodynia (PVD). |
| Single-Digit Exam | Identifies hypertonicity, trigger points, or "Jump Sign" (flinch). |
| Transvaginal US | First-line for cysts/fibroids. Note: Often misses superficial endometriosis. |
Red Flag Triage
Urgent Care (A&E) required for:
- Sudden "Thunderclap" pain.
- Heavy bleeding (soaking 1 pad/hour).
- Fever (>38°C) with pelvic pain.
- Cauda Equina signs (Saddle numbness/incontinence).
4.0 Foundational and Evidence-Based Therapies
Multimodal care is the gold standard.
Exploring advanced options?
Get Support5.0 Regenerative Procedures: Evidence Review
These are generally considered adjunctive. Regulatory status varies.
| Procedure | Mechanism | Evidence Status |
|---|---|---|
| Vaginal Laser (CO2) | Thermal micro-injury stimulates collagen. | Emerging. NICE: Safety established but long-term efficacy evidence "inadequate." |
| PRP (O-Shot) | Growth factors stimulate regeneration. | Experimental. Promising for Lichen Sclerosus and scars. |
| Emsella Chair | HIFEM induces muscle contractions. | Evidence-based for Incontinence. Sexual improvement is secondary. |
Synergistic Protocols
- 1. Estrogen Priming + Laser: Estrogen hydrates tissue first, improving laser target and collagen yield.
- 2. Hardware + Software: Emsella builds muscle (hardware); Physio teaches coordination (software).
- 3. Regenerate + Retrain: PRP improves tissue quality; Dilators then retrain the fear response.
Safety & Consent Standards
We adhere to the Montgomery Standard for consent and use only UKCA/CE marked devices.
6.0 Safety, Consent, and Management
Medical Device Safety
UKCA/CE Marks: Mandatory. "FDA Approval" is meaningless in the UK.
Intended Use: Beware "off-label" use (e.g., skin laser used internally).
Aftercare Protocols
- Laser: Abstain 5-7 days.
- Fillers: Abstain 3-5 days (prevent migration).
- PRP: Avoid NSAIDs (Ibuprofen) for 7 days pre/post (blocks platelets).
Self-Management Tools
- Traffic Light System: Green/Amber/Red communication for patient control.
- Sexual Menu: Redefining intimacy beyond penetration to reduce anxiety.
Disclaimer: This content is for informational purposes only and does not constitute medical advice. Consult a healthcare professional for diagnosis and treatment.
